Collaboration of Cardiac Surgery & Urology treating A Patient of Renal Cell Carcinoma with Inferior Vena Cava Infiltration
Dr Rezaul Hassan, Dr M Zahid Hasan
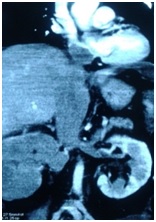
A 48 year old hypertensive female presented with a 2 month history of generalized weakness, loss of appetite, weight loss and abdominal discomfort. On physical examination the patient was anaemic, icteric with mild tachycardia. Her laboratory examination revealed anemia, elevated level of serum bilirubin and liver enzymes (ALT, AST, Alkaline Phosphatase), raised serum LDH, features of coagulopathy (raised APTT, INR, FDP, D-dimer). Abdominal ultrasonography (USG) showed right renal mass, dilated inferior vena cava (IVC) with echo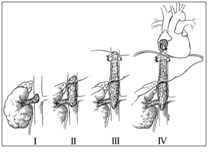 genic thrombus in right renal vein and IVC extending up to the heart. Contrast CT scan of the whole abdomen and chest showed right kidney was replaced by a heterogeneous density soft tissue mass with extension into the right renal vein, IVC, proximal part of left renal vein, confluence of hepatic vein and up to the right atrium (RA) (Fig-1). There were no hepatic lesion and no paraaortic lymphadenopathy. There were no lesion found in intrathoracic great vessels and lungs.
genic thrombus in right renal vein and IVC extending up to the heart. Contrast CT scan of the whole abdomen and chest showed right kidney was replaced by a heterogeneous density soft tissue mass with extension into the right renal vein, IVC, proximal part of left renal vein, confluence of hepatic vein and up to the right atrium (RA) (Fig-1). There were no hepatic lesion and no paraaortic lymphadenopathy. There were no lesion found in intrathoracic great vessels and lungs.
The patient’s condition was deteriorating rapidly due to hepatic encephalopathy. She was shifted to ICU for necessary support and close monitoring. On the following day a medical board was arranged involving all allied Consultants; decision was taken for Radical Nephrectomy with Thombectomy from all extension with hypothermic cardiopulmonary bypass with cardiac arrest.
 Surgical procedure was planned in collaboration with a urological team aiming complete resection of primary tumor, paraaortic lymphadenectomy (if present) and removal of IVC thrombus extending to RA with the help of cardiopulmonary bypass. The right kidney was mobilized by sharp and blunt dissection through a rooftop incision. IVC felt firm with tumor thrombus within. Right nephrectomy was performed. IVC was mobilized gently and taped. Cardiopulmonary bypass (CPB) was established by aortic cannula (24 Fr), venous cannulas were placed in the superior vena cava directly (24 Fr) and right femoral vein (22 Fr). Under moderate hypothermia and low flow, the ascending aorta was cross-clamped and cold blood cardioplegic solution was administered for myocardial protection antegradely. After arresting heart, RA was opened and the mass was seen just reaching the IVC-RA junction. The tumor thrombus was removed through RA from IVC and hepatic vein level (Fig-2). Abdominal IVC was opened and the entire residual mass was removed from below, small amount of thrombus was also removed from left renal vein. After IVC and RA were closed, the patient was gradually weaned from bypass and cannulas were removed. Total bypass time was 155 minutes and total cross clamp time was 85 minutes. After 7 hour long operation patient was shifted to CICU where she was drowsy for two days requiring ventilator support. On 5th POD onward she was completely awake and alert, taking food orally. On 9th POD LFT, RFT, CBC electrolyte, CXR, coagulation profile and abdominal USG, all showed normal findings.
Surgical procedure was planned in collaboration with a urological team aiming complete resection of primary tumor, paraaortic lymphadenectomy (if present) and removal of IVC thrombus extending to RA with the help of cardiopulmonary bypass. The right kidney was mobilized by sharp and blunt dissection through a rooftop incision. IVC felt firm with tumor thrombus within. Right nephrectomy was performed. IVC was mobilized gently and taped. Cardiopulmonary bypass (CPB) was established by aortic cannula (24 Fr), venous cannulas were placed in the superior vena cava directly (24 Fr) and right femoral vein (22 Fr). Under moderate hypothermia and low flow, the ascending aorta was cross-clamped and cold blood cardioplegic solution was administered for myocardial protection antegradely. After arresting heart, RA was opened and the mass was seen just reaching the IVC-RA junction. The tumor thrombus was removed through RA from IVC and hepatic vein level (Fig-2). Abdominal IVC was opened and the entire residual mass was removed from below, small amount of thrombus was also removed from left renal vein. After IVC and RA were closed, the patient was gradually weaned from bypass and cannulas were removed. Total bypass time was 155 minutes and total cross clamp time was 85 minutes. After 7 hour long operation patient was shifted to CICU where she was drowsy for two days requiring ventilator support. On 5th POD onward she was completely awake and alert, taking food orally. On 9th POD LFT, RFT, CBC electrolyte, CXR, coagulation profile and abdominal USG, all showed normal findings.
 Postoperative Venous Doppler showed no residual thrombus in venous system. The specimen (Fig-3) showed involvement of the perinephric fat as well as ureteric lumen. Patient did not have any complications such as pneumonia, wound infection, deep venous thrombosis rather improvement of hepatic dysfunction in the immediate post operative period. The patient was discharged from hospital on the 12th post-operative day. Her histopathology report showed Papillary renal cell carcinoma TNM stage T3b Nx Mx involving kidney, renal capsule, perinephric fat, renal pelvis and proximal ureter, paraaortic Lymph node and Tumor thrombus. FDG based PET scan done 9 week after surgery showed hyper metabolic spot only in sixth segment of Liver, IVC and Left Renal Vein. She further was planned for Targeted Therapy Pazopanib as follow up treatment.
Postoperative Venous Doppler showed no residual thrombus in venous system. The specimen (Fig-3) showed involvement of the perinephric fat as well as ureteric lumen. Patient did not have any complications such as pneumonia, wound infection, deep venous thrombosis rather improvement of hepatic dysfunction in the immediate post operative period. The patient was discharged from hospital on the 12th post-operative day. Her histopathology report showed Papillary renal cell carcinoma TNM stage T3b Nx Mx involving kidney, renal capsule, perinephric fat, renal pelvis and proximal ureter, paraaortic Lymph node and Tumor thrombus. FDG based PET scan done 9 week after surgery showed hyper metabolic spot only in sixth segment of Liver, IVC and Left Renal Vein. She further was planned for Targeted Therapy Pazopanib as follow up treatment.